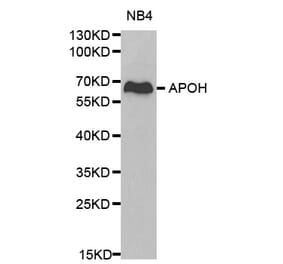
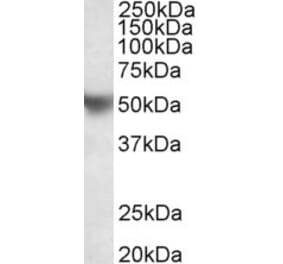
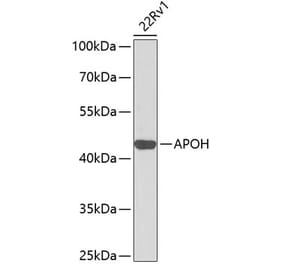
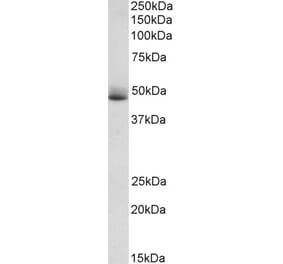
Western blot analysis of human plasma (0.1 µl and 0.01 µl) using 1 µg/ml Anti-Apo-H Antibody [H219] (A269918), followed by SA-ALP and BCIP/NBT-plus substrate.
Publishing research using Anti-Apo-H Antibody [H219] (A269918)? Please let us know so that we can list the citation on this page.
Alternative products to Anti-Apo-H Antibody [H219] (A269918)


![WB - Anti-Apo-H Antibody [H219] (A269918) - Antibodies.com](https://cdn.antibodies.com/image/catalog/269/A269918_2.png?profile=product_top)
![WB - Anti-Apo-H Antibody [H219] (A269918) - Antibodies.com](https://cdn.antibodies.com/image/catalog/269/A269918_2.png?profile=product_top_thumb)
![WB - Anti-Apo-H Antibody [H219] (A269918) - Antibodies.com](https://cdn.antibodies.com/image/catalog/269/A269918_2.png?profile=product_image)

![Immunohistochemistry - Anti-Apo-H Antibody [ID2] (A280698) - Antibodies.com](https://cdn.antibodies.com/image/catalog/280/A280698_1.jpg?profile=product_alternative)