| Sample Type | n | Range | Average |
|---|---|---|---|
| Serum | 5 | 80% - 102% | 91% |
| EDTA Plasma | 5 | 81% - 99% | 90% |
| Heparin Plasma | 5 | 80% - 89% | 84% |
| Sample Type | 1:2 | 1:4 | 1:8 | 1:16 |
|---|---|---|---|---|
| Serum (n=5) | 87-91% | 87-107% | 74-101% | 92-97% |
| EDTA Plasma (n=5) | 90-105% | 84-101% | 90-101% | 79-108% |
| Heparin Plasma (n=5) | 84-95% | 92-105% | 82-105% | 89-91% |
| Item | Quantity | Storage |
|---|---|---|
| Pre-Coated 96 Well Microplate | 12 x 8 Well Strips | -20°C |
| Lyopholized Standard | 2 Vials | -20°C |
| Detection Solution A | 70μl | -20°C |
| Detection Solution B | 120µl | -20°C |
| Wash Buffer (30X) | 20ml | +4°C |
| Sample Dilution Buffer | 45ml | -20°C |
| TMB Substrate | 9ml | +4°C |
| Stop Solution | 6ml | +4°C |
| Plate Sealers | 5 Adhesive Strips | - |
Background: Atrial fibrillation (AF) is common complication of heart failure with preserved ejection fraction (HFpEF) that sufficiently intervenes in the prognosis. The aim of the study is a) to investigate the possible discriminative value of adropin for newly onset AF in patients with HFpEF without a previous history of AF and who are being treated in accordance with conventional guideline and b) to compare it with predictive potencies of conventionally used predictors.
Methods: A total of 953 patients with HFpEF who had sinus rhythm on ECG were enrolled in the study. The course of the observation was 3 years. Echocardiography and assessment of conventional hematological, biochemical parameters and biomarker assay including N-terminal brain natriuretic pro-peptide (NT-proBNP), high-sensitivity cardiac troponin T, tumor necrosis factor-alpha, high-sensitivity C-reactive protein (hs-CRP), galectin-3, interleukin-6, soluble suppressor tumorigenisity-2 (sST2) and adropin, were performed at baseline.
Results: Incident atrial fibrillation was found in 172 patients with HFpEF, whereas 781 had sinus rhythm. In unadjusted rough Cox regression model, age = 75 years, type 2 diabetes mellitus, chronic kidney disease (CKD) stages 1-3, left atrial volume index (LAVI) = 40 mL/m2, NT-proBNP = 1440 pmol/mL, hs-CRP = 5.40 mg/L, adropin = 2.95 ng/mL, sST2 = 15.5 ng/mL were identified as the predictors for new onset AF in HFpEF patients. After adjusting for age = 75 years, a presence of type 2 diabetes mellitus and CKD stages 1-3, the levels of NT-proBNP = 1440 pmol/mL and adropin = 2.95 ng/mL were independent predictors of new onset AF in patients HFpEF. We also found that discriminative value of adropin was superior to NT-proBNP, while adding adropin to NT-proBNP did not improve predictive information of adropin alone.
Conclusions: adropin = 2.95 ng/mL presented more predictive information than NT-proBNP = 1440 pmol/mL alone for new cases of AF in symptomatic patients with HFpEF, whereas the combination of both biomarkers did not improve the predictive ability of adropin alone.
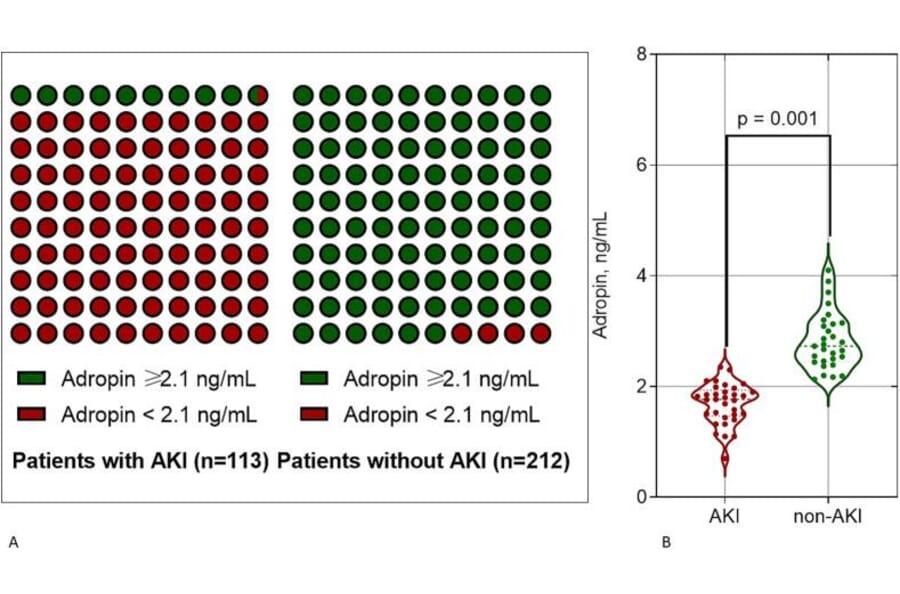
Background: Patients with acutely decompensated heart failure (ADHF) demonstrated a high risk of acute kidney injury (AKI) and its transition to acute kidney disease after diuretic therapy to reach euvolemic status. The purpose of the study was to investigate whether circulating levels of adropin predict AKI in ADHF patients after decongestive therapy.
Material and methods: A total of 325 individuals fulfilling the inclusion criteria of ADHF were consecutively enrolled from October 2020 to October 2024. The study was designed as prospective cohort study. The congestion was assessed using Framingham criteria of congestion (Framingham heart failure score = 2). Patients with AHDF were divided into 2 groups according to the presence of AKI (n = 113) and without AKI (n = 212). Circulating levels of N-terminal brain natriuretic pro-peptide (NT-proBNP), high-sensitivity C-reactive protein, high-sensitive troponin T, interleukin-6, tumor necrosis factor-alpha, soluble suppression of tumorigenicity-2, procalcitonin were measured. Predictors of AKI were identified using univariate and multivariate logistic regression analysis.
Results: We found that the presence of atrial fibrillation, urinary albumin/creatinine ratio (UACR) =16.5 mg/g Cr, serum levels of adropin<2.1 ng/mL and NT-proBNP =19,540 pmol/mL were independent predictors for AKI in patients with ADHF. UACR and atrial fibrillation revealed a strict similarity in prediction of AKI, whereas discriminative ability of adropin<2.1 ng/mL were higher to NT-proBNP =19,540 pmol/mL. The combined predictive model (low levels of adropin + higher levels of NT-proBNP) showed significantly better discriminatory power compared to other models.
Conclusion: Low levels of adropin<2.1 ng/mL on hospital admission in patients with ADHF can predict AKI and that its predictive ability was significantly higher compared with the conventionally used urinary albumin/creatinine ratio and NT-proBNP. Adropin may add predictive information to NT-proBNP for AKI in individuals with ADHF.