| Sample Type | n | Range | Average |
|---|---|---|---|
| Serum | 10 | 85% - 103% | 94% |
| EDTA Plasma | 10 | 86% - 105% | 96% |
| Heparin Plasma | 10 | 90% - 104% | 100% |
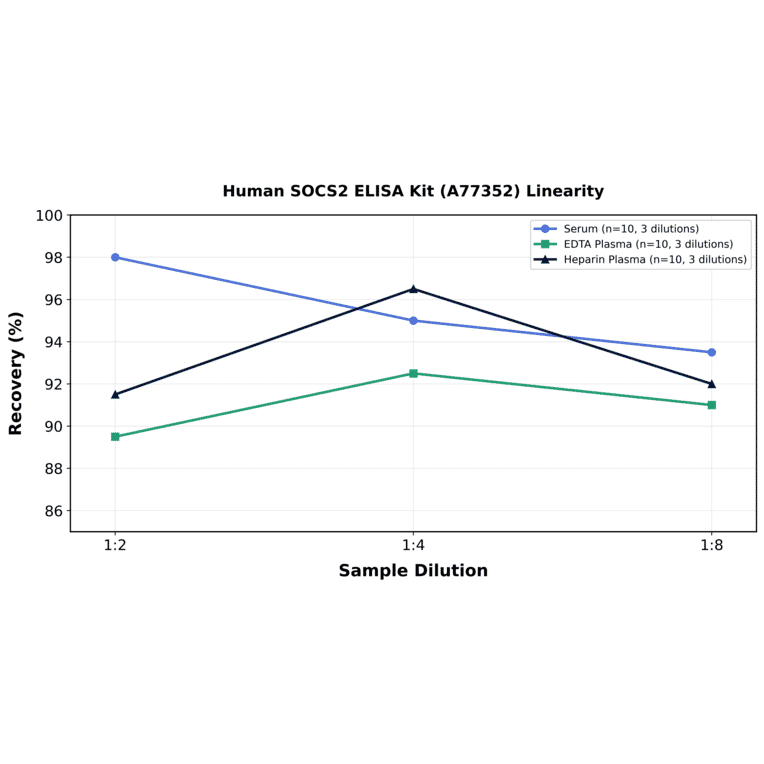
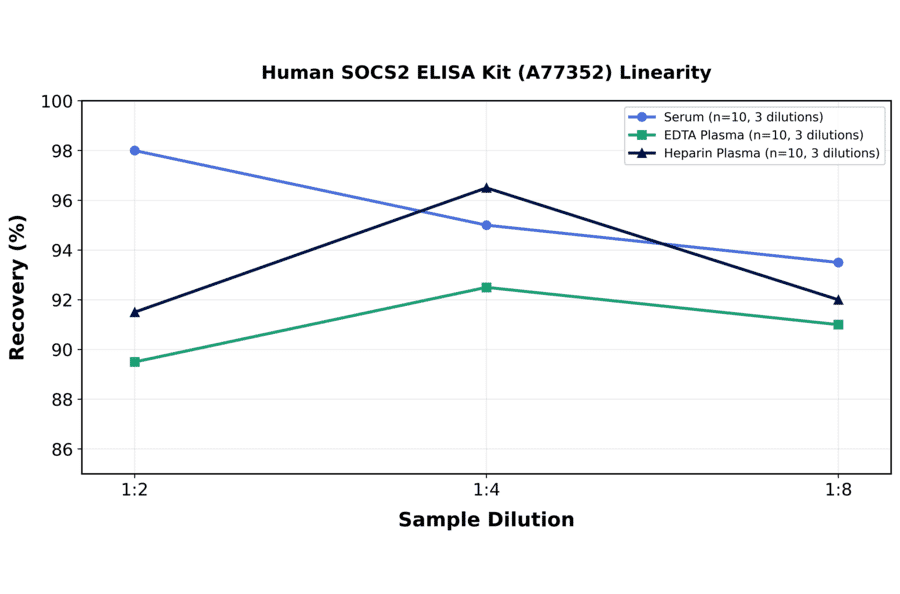
| Sample Type | n | 1:2 | 1:4 | 1:8 |
|---|---|---|---|---|
| Serum | 10 | 91-105% | 89-101% | 85-102% |
| EDTA Plasma | 10 | 83-96% | 86-99% | 86-96% |
| Heparin Plasma | 10 | 84-99% | 88-105% | 84-100% |
| Item | Quantity | Storage |
|---|---|---|
| Pre-Coated 96 Well Microplate | 12 x 8 Well Strips | +4°C |
| Lyopholized Standard | 2 Vials | +4°C |
| Sample Dilution Buffer | 20ml | +4°C |
| Biotinylated Detection Antibody | 120µl | +4°C |
| Antibody Dilution Buffer | 10ml | +4°C |
| HRP-Streptavidin Conjugate | 120µl | +4°C |
| SABC Dilution Buffer | 10ml | +4°C |
| TMB Substrate | 10ml | +4°C |
| Stop Solution | 10ml | +4°C |
| Wash Buffer (25X) | 30ml | +4°C |
| Plate Sealers | 5 Adhesive Strips | - |
| Foil Pouch | 1 Zip-Sealed Pouch | - |
Background: Growth failure is a common and serious complication of chronic kidney disease (CKD) in children, resulting from numerous factors, including growth hormone (GH) resistance. Suppressor of cytokine signaling 2 (SOCS2), a negative regulator of GH signaling, has been implicated in growth regulation but has not been previously studied in pediatric CKD.
Methods: In this cross-sectional study, we assessed serum SOCS2 concentrations in 55 children with CKD (stages 2-5) and 27 age- and sex-matched healthy controls using a high-sensitivity ELISA. We evaluated anthropometric parameters, kidney function, and biochemical markers. Associations between SOCS2 levels and growth (height standard deviation scores, HtSDS) were analyzed using correlation and multivariate regression models.
Results: SOCS2 levels were significantly higher in children with CKD compared to controls (median 1526.5 vs. 1294.6 pg/ml, p < 0.001). In patients with CKD, SOCS2 negatively correlated with HtSDS (r = -0.30, p = 0.029). In multivariate analysis, SOCS2 was an independent predictor of lower HtSDS alongside eGFR. SOCS2 concentrations were higher in short-statured children, and ROC analysis showed acceptable diagnostic performance for predicting short stature (AUC 0.78, 95% CI 0.64-0.91; 79.5% sensitivity, 68.8% specificity).
Conclusions: Circulating SOCS2 levels are elevated in pediatric CKD and independently associated with growth impairment, suggesting its potential link to GH resistance, which is typical of CKD. SOCS2 might be a potential new marker of growth retardation. Further longitudinal studies are needed to explore its predictive value for longitudinal growth and GH treatment response.