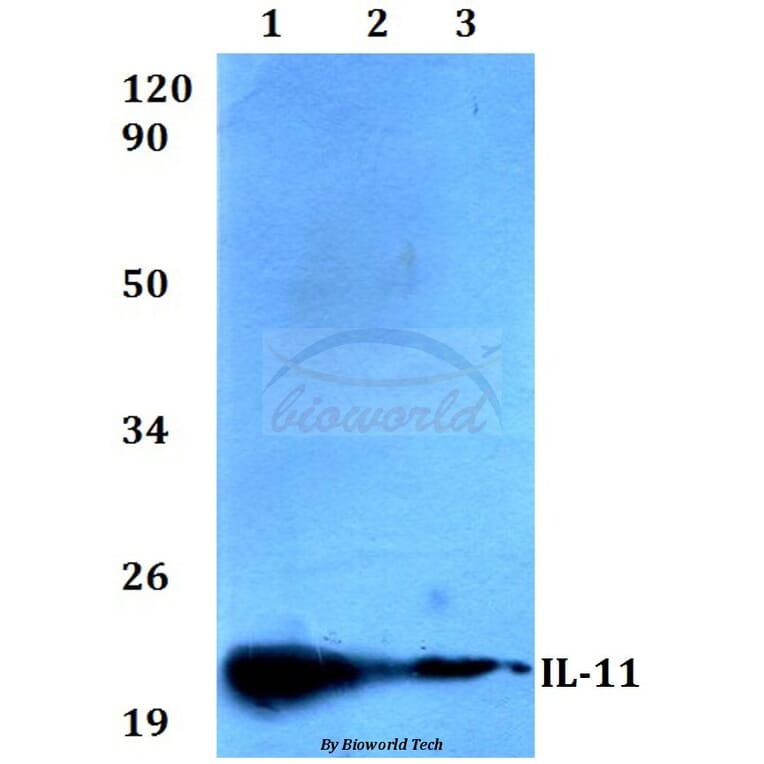
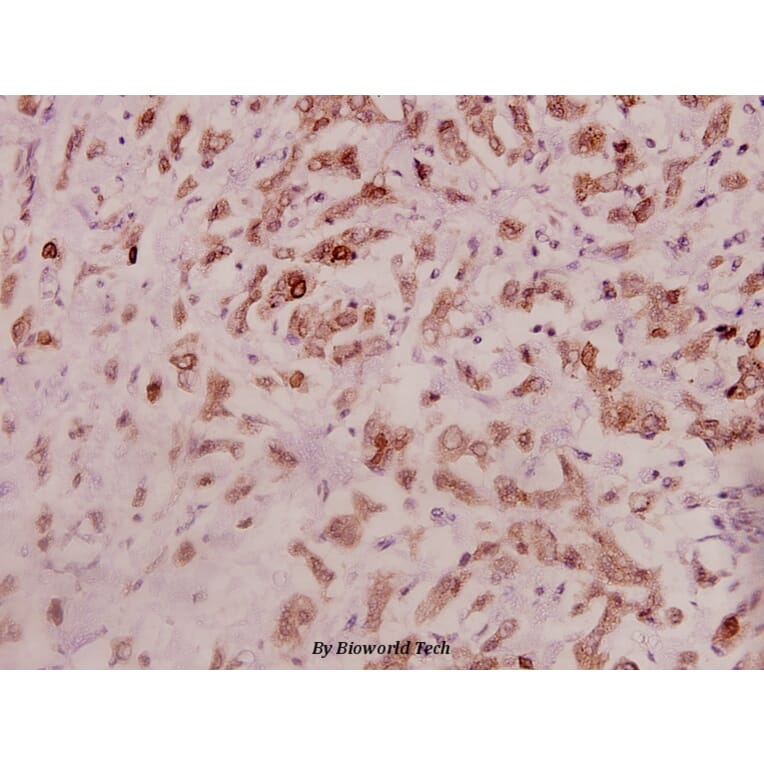
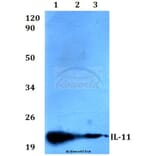
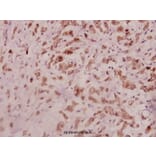
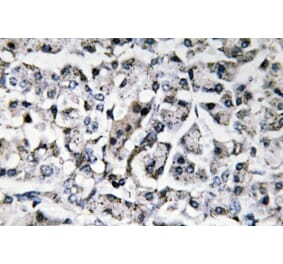
IL-11 (G27) pAb detects endogenous levels of IL-11 protein.
Applications
WB, IHC
Reactivity
Human, Mouse, Rat
Immunogen
Synthetic peptide, corresponding to the N-terminus of Human IL-11.
Host
Rabbit
Clonality
Polyclonal
Conjugate
Unconjugated
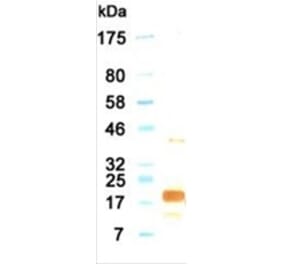
Molecular Weight
~ 21 kDa
Purity
The antibody was affinity-purified from rabbit antiserum by affinity-chromatography using epitope-specific immunogen and the purity is > 95% (by SDS-PAGE).
Product Form
1 mg/ml in Phosphate buffered saline (PBS) with 0.05% sodium azide, approx. pH 7.2.
Recombinant humanantibody to IL-11 for use as a research grade BI 765423 biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.
Recombinant human monoclonal antibody to IL-11 for use as a research grade Anti-Human IL11 Antibody for ELISA, Functional Studies and in vivo Research.
Recombinant humanantibody to IL-11 for use as a research grade BI 765423 biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.
Recombinant human monoclonal antibody to IL-11 for use as a research grade Anti-Human IL11 Antibody for ELISA, Functional Studies and in vivo Research.




![SDS-PAGE - Anti-IL-11 Antibody [BI 765423] Biosimilar - BSA and Azide free (A340848) - Antibodies.com](https://cdn.antibodies.com/image/catalog/340/A340848_1.jpg?profile=product_alternative)
![SDS-PAGE - Anti-IL-11 Antibody [X23] Biosimilar - BSA and Azide free (A339283) - Antibodies.com](https://cdn.antibodies.com/image/catalog/339/A339283_1.jpg?profile=product_alternative)
![SDS-PAGE - Anti-IL-11 Antibody [Enx18A] Biosimilar - BSA and Azide free (A340850) - Antibodies.com](https://cdn.antibodies.com/image/catalog/340/A340850_1.jpg?profile=product_alternative)
![ELISA - Anti-IL-11 Antibody [D08-4C12] (A280203) - Antibodies.com](https://cdn.antibodies.com/image/catalog/280/A280203_1.jpg?profile=product_alternative)