Unconjugated
Atopic dermatitis is a common pruritic skin disease in which barrier dysfunction and cutaneous inflammation contribute to pathogenesis. Mechanisms underlying the associated inflammation are not fully understood, and although Langerhans cells expressing the nonclassical major histocompatibility complex (MHC) family member CD1a are known to be enriched within lesions, their role in clinical disease pathogenesis has not been studied. We observed that house dust mite (HDM) allergen generates neolipid antigens presented by CD1a to T cells in the blood and skin lesions of affected individuals. HDM-responsive CD1a-reactive T cells increased in frequency after birth in individuals with atopic dermatitis and showed rapid effector function, consistent with antigen-driven maturation. In HDM-challenged human skin, we observed phospholipase A2 (PLA2) activity in vivo. CD1a-reactive T cell activation was dependent on HDM-derived PLA2, and such cells infiltrated the skin after allergen challenge. Moreover, we observed that the skin barrier protein filaggrin, insufficiency of which is associated with atopic skin disease, inhibited PLA2 activity and decreased CD1a-reactive PLA2-generated neolipid-specific T cell activity from skin and blood. The most widely used classification schemes of hypersensitivity suggest that nonpeptide stimulants of T cells act as haptens that modify peptides or proteins; however, our results show that HDM proteins may also generate neolipid antigens that directly activate T cells. These data define PLA2 inhibition as a function of filaggrin, supporting PLA2 inhibition as a therapeutic approach.
Alterations in hematopoietic microenvironment of acute lymphoblastic leukemia patients have been claimed to occur, but little is known about the components of marrow stroma in these patients. In this study, we characterized mesenchymal stromal cells (MSCs) isolated from bone marrow (BM) of 45 pediatric patients with acute lymphoblastic leukemia (ALL-MSCs) at diagnosis (day+0) and during chemotherapy treatment (days: +15; +33; +78), the time points being chosen according to the schedule of BM aspirates required by the AIEOP-BFM ALL 2009 treatment protocol. Morphology, proliferative capacity, immunophenotype, differentiation potential, immunomodulatory properties and ability to support long-term hematopoiesis of ALL-MSCs were analysed and compared with those from 41 healthy donors (HD-MSCs). ALL-MSCs were also genetically characterized through array-CGH, conventional karyotyping and FISH analysis. Moreover, we compared ALL-MSCs generated at day+0 with those isolated during chemotherapy. Morphology, immunophenotype, differentiation potential and in vitro life-span did not differ between ALL-MSCs and HD-MSCs. ALL-MSCs showed significantly lower proliferative capacity (p<0.001) and ability to support in vitro hematopoiesis (p = 0.04) as compared with HD-MSCs, while they had similar capacity to inhibit in vitro mitogen-induced T-cell proliferation (p = N.S.). ALL-MSCs showed neither the typical translocations carried by the leukemic clone (when present), nor other genetic abnormalities acquired during ex vivo culture. Our findings indicate that ALL-MSCs display reduced ability to proliferate and to support long-term hematopoiesis in vitro. ALL-MSCs isolated at diagnosis do not differ from those obtained during treatment.









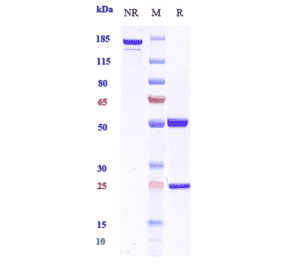
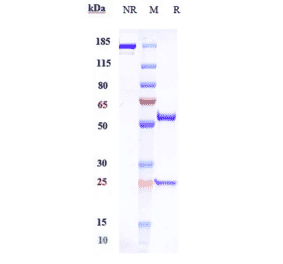
![SDS-PAGE - Anti-GM-CSF Antibody [Research Grade Biosimilar] - Low endotoxin, Azide free (A324043) - Antibodies.com](https://cdn.antibodies.com/image/catalog/324/A324043_1.jpg?profile=product_alternative)
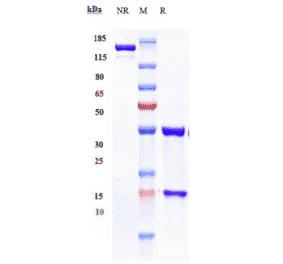
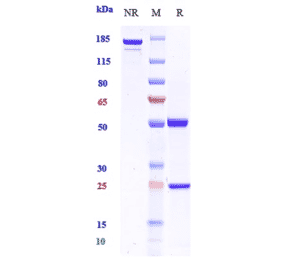
![SDS-PAGE - Anti-GM-CSF Antibody [BVD2-21C11] (A248272) - Antibodies.com](https://cdn.antibodies.com/image/catalog/248/A248273_1.jpg?profile=product_alternative)
![SDS-PAGE - Anti-GM-CSF Antibody [BVD2-21C11] - BSA and Azide free (A251454) - Antibodies.com](https://cdn.antibodies.com/image/catalog/251/A251455_1.jpg?profile=product_alternative)
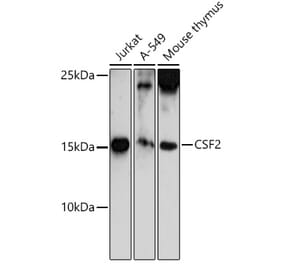
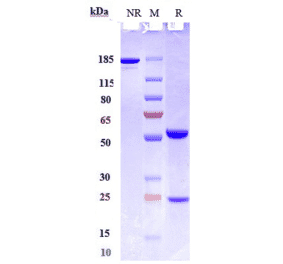
![SDS-PAGE - Anti-GM-CSF Antibody [CSF2/3403] (A248272) - Antibodies.com](https://cdn.antibodies.com/image/catalog/248/A248272_1.jpg?profile=product_alternative)
![SDS-PAGE - Anti-GM-CSF Antibody [CSF2/3403] - BSA and Azide free (A251454) - Antibodies.com](https://cdn.antibodies.com/image/catalog/251/A251454_1.jpg?profile=product_alternative)