Principle of Assay
This SAA enzyme-linked immunosorbent assay (ELISA) applies a technique called quantitative sandwich immunoassay. The microtiter plate provided in this kit has been pre-coated with a monoclonal antibody specific for SAA. Standards or samples are then added to the appropriate microtiter plate wells and incubated. SAA if present, will bind and become immobilized by the antibody pre-coated on the wells. The microtiter plate wells are thoroughly washed to remove any unbound SAA and other components of sample. In order to quantitate the amount of SAA present in the sample, a standardized preparation of horseradish peroxidase (HRP)-conjugated monoclonal antibody specific for SAA is added to each well to "sandwich" the SAA immobilized during the first incubation. The microtiter plate then undergoes a second incubation. The wells are thoroughly washed to remove all unbound HRP-conjugated antibodies and a TMB (3,3'5,5' tetramethyl-benzidine) substrate solution is added to each well. The enzyme (HRP) and substrate solution are allowed to react over a short incubation period. Only those wells that contain SAA and enzyme-substrate reaction will exhibit a change in colour. The enzyme-substrate reaction is terminated by the addition of sulphuric acid solution and the colour change measured spectrophotometrically at a wavelength of 450 nm ± 2 nm.
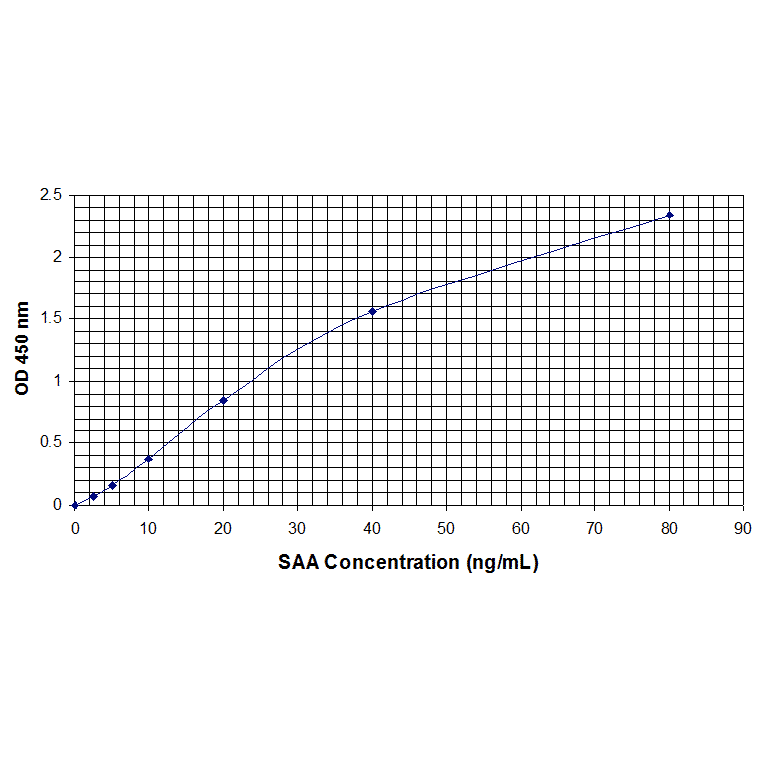
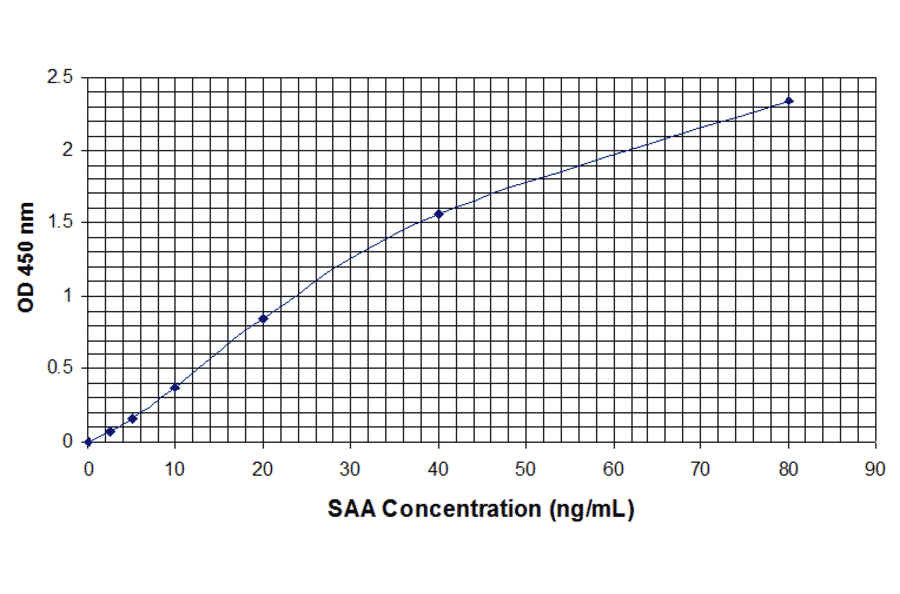
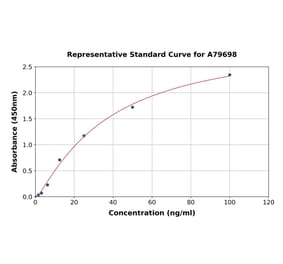
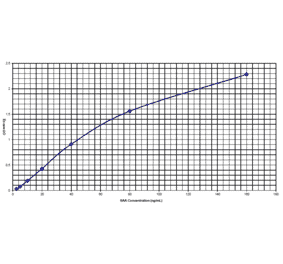
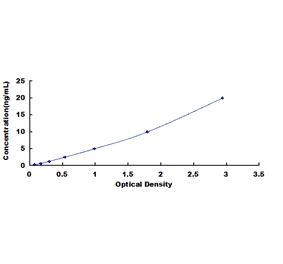
In order to measure the concentration of SAA in the samples, this kit includes two calibration diluents (Calibrator Diluent I for serum/plasma testing and Calibrator Diluent II for cell culture supernatant testing). According to the testing system, the provided standard is diluted (2-fold) with the appropriate Calibrator Diluent and assayed at the same time as the samples. This allows the operator to produce a standard curve of Optical Density (O.D) versus SAA (ng/mL). The concentration of SAA in the samples is then determined by comparing the O.D. of the samples to the standard curve.