Recombinant humanized monoclonal antibody to IL-5 for use as a research grade Mepolizumab biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.
Recombinant human monoclonal antibody to IL-5 for use as a research grade Varokibart biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.
Recombinant humanized monoclonal antibody to IL-5 for use as a research grade Reslizumab biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.
Recombinant humanized monoclonal antibody to IL-5 for use as a research grade Mepolizumab biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.
Recombinant human monoclonal antibody to IL-5 for use as a research grade Varokibart biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.
Recombinant humanized monoclonal antibody to IL-5 for use as a research grade Reslizumab biosimilar for ELISA, Flow Cytometry, Functional Studies and in vivo Research.



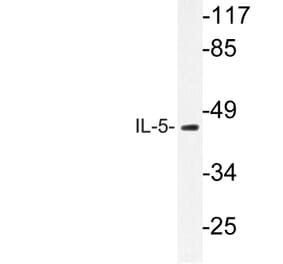
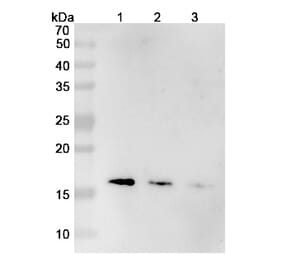
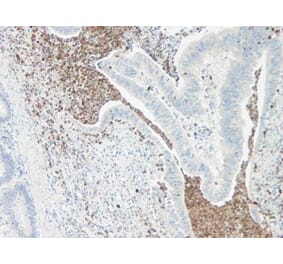
![Immunohistochemistry - Anti-IL-5 Antibody [IL5/4161] (A277671) - Antibodies.com](https://cdn.antibodies.com/image/catalog/277/A277671_1.jpg?profile=product_alternative)
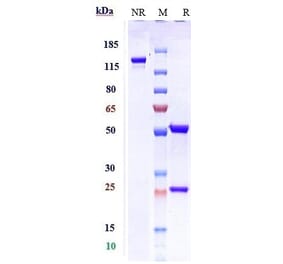
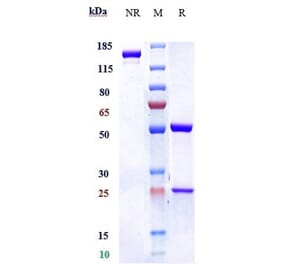
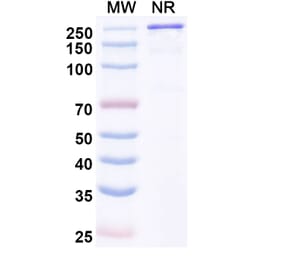
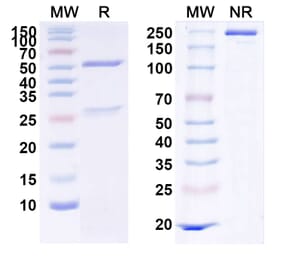
![SDS-PAGE - Anti-IL-5 Antibody [Research Grade Biosimilar] - Low endotoxin, Azide free (A324095) - Antibodies.com](https://cdn.antibodies.com/image/catalog/324/A324095_1.jpg?profile=product_alternative)
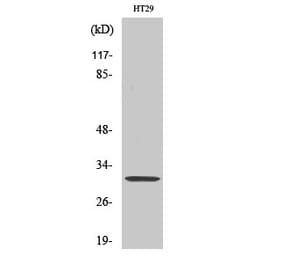
![Immunohistochemistry - Anti-IL-5 Antibody [IL5/4161] - BSA and Azide free (A278259) - Antibodies.com](https://cdn.antibodies.com/image/catalog/278/A278259_1.jpg?profile=product_alternative)