Unconjugated
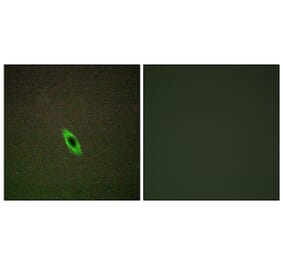
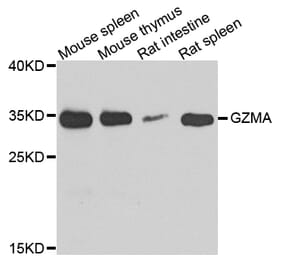
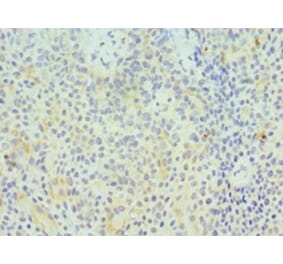
The pleiotropic cytokine interleukin (IL)-10 is best characterized by its ability to downregulate inflammation and promote peripheral tolerance. On the other hand, IL-10 was also found to maintain the effector response of CD8+ T cells and promote the expansion of tumor-resident CD8+ T cells. In diffuse large B cell lymphoma (DLBCL), the role of IL-10 has been characterized in tumor cells but not in CD8+ T cells. We found that CD8+ T cells in DLBCL presented robust interferon (IFN)-? expression early during TCR-activation but could not maintain this response later on, which was characterized by significantly lower CD8+ T cell degranulation and higher apoptosis. These observations were associated with higher PD-1 expression in DLBCL CD8+ T cells. Furthermore, the PD-1+ cells were strongly enriched in the IFN-?+, but not the IFN-?-, fraction. Interestingly, exogenous IL-10 significantly improved the survival of DLBCL CD8+ T cells, and resulted in significantly higher IFN-?, ganzyme A and granzyme B expression in the absence of CD19+ tumor cells, and significantly improved CD8+ T cell-mediated specific lysis of CD19+ tumor cells. IL-10 did not alter the expression of PD-1 in DLBCL CD8+ T cells, but curiously, IL-10-treated DLBCL CD8+ T cells were less susceptible to PD-L1-mediated apoptosis. We then demonstrated that IL-10 treatment significantly elevated the expression of pro-survival factor Bcl-2. Blocking IL-10 resulted in higher apoptosis, fewer IFN-?+ CD8+ T cells, and lower Bcl-2 expression. IL-10 also significantly increased STAT3, but not STAT1, phosphorylation in CD8+ T cells. Together, these results suggested that IL-10 could enhance CD8+ T cell inflammation in DLBCL patients.
Diffuse large B-cell lymphoma (DLBCL) is a common and aggressive subtype of non-Hodgkin's lymphomas, with limited treatment options in refractory and relapsed patients. Growing evidence supports the notion that CD8+ T cell immunity could be utilized to eliminate B cell lymphomas. CXCR5+CD8+ T cell is a novel cell subtype and share CXCR5 expression with CD19+ tumor cells. In this study, we investigated the frequency and function of existing CXCR5+CD8+ T cells in DLBCL patients. We found that DLBCL patients as a group demonstrated significantly higher level of CXCR5+CD8+ T cells than healthy individuals, with huge variability in each patient. Using anti-CD3/CD28-stimulated CD8+ T cells as effector (E) cells and autologous CD19+ tumor cells as target (T) cells, at high E:T ratio, no difference between the intensities of CXCR5+CD8+ T cell- and CXCR5-CD8+ T cell-mediated cytotoxicity were observed. However, at intermediate and low E:T ratios, the CXCR5+CD8+ T cells presented stronger cytotoxicity than CXCR5-CD8+ T cells. The expressions of granzyme A, granzyme B, and perforin were significantly higher in CXCR5+CD8+ T cells than in CXCR5-CD8+ T cells, with no significant difference in the level of degranulation. Tumor cells in DLBCL were known to secrete high level of interleukin 10 (IL-10). We therefore blocked the IL-10/IL-10R pathway, and found that the expressions of granzyme A, granzyme B, and perforin by CXCR5+CD8+ T cells were significantly elevated. Together, these results suggest that CXCR5+CD8+ T cells are potential candidates of CD8+ T cell-based immunotherapies, could mediate elimination of autologous tumor cells in DLBCL patients, but are also susceptible to IL-10-mediated suppression.


![Flow Cytometry - Anti-Granzyme A Antibody [CB9] (A285846) - Antibodies.com](https://cdn.antibodies.com/image/catalog/285/A285847_1.jpg?profile=product_alternative)